HypoAdrenal Shock is life-threatening exacerbation of adrenal insufficiency (AI) when an increased hormone demand fails to increase the supply. AI is specifically deficiency of adrenal gland hormone production in the cortex.
Physiology
Take Home:

Physiology
The adrenal gland is made up of the cortex and medulla producing steroid hormones and catecholamines respectively. The adrenal cortex
produces three categories of steroids:


Clinical Features
Secondary adrenal insufficiency presents with symptoms of diminished cortisol (weight loss, lethargy, weakness, confusion, anorexia, GI distress, abdominal pain). Typically secondary AI presents as Hypoglycemia, Hypo/HyperNa, Hypokalemia, Hypotension.
Treatment
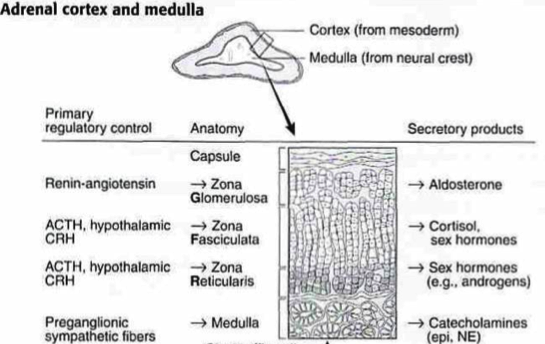
- Glucocorticoids (cortisol) from zone fasciculate (Under Hypothalamus/Pitiutary control)
- Mineralocorticoids (aldosterone) from zona glomerulosa (Under control of RAAS)
- Gonadocorticoids (sex hormones) from zone reticular (Under Hypothalamus/Pitiutary control)
- Catecholamines (adrenaline, noradrenaline and dopamine) from adrenal medulla
Functions of steroid hormones:
Glucocorticoids: Cortisol secretion is under control of hypothalmaic-pitiutary axis. Daily cortisol requirement is about 20 mg of hydrocortisone. Cortisol facilitates (Permissive action of glucocorticoids) the stress
response by affecting the heart, vascular bed, water excretion, electrolyte
balance, potentiation of catecholamine action, and control of water distribution. It affects metabolism by stimulating glycogenolysis and glyconeogenesis. It is also involved in immunologic/inflammatory responses.
Mineralocorticoids : Aldosterone secretion is controlled primarily by the renin-angio-
tensin system (unlike cortisol) and serum potassium concentration. Aldosterone maintains sodium and potassium plasma concentrations. It regulates extracellular volume and controls sodium and water
balance.
Gonadocorticoids: Promote the development of sex characteristics such as axillary and pubic hair and libido.

There are two types of Adrenal deficiency syndromes:
Primary AI (Addison’s disease) i.e. intrinsic adrenal gland dysfunction that results in decreased Glucocorticoids (cortisol), Mineralocorticoids (aldosterone), and sex hormones production. Fortunately, primary AI is a rare disease. Approximately 90% of the gland must be destroyed to manifest symptoms. Autoimmune
disorders and infections such as tuberculosis are responsible for most cases of primary adrenal insufficiency. Infiltrative diseases such as amyloidosis, hemosiderosis, Thrombosis and/or haemorrhage (anticoagulation therapy, sepsis, DIC, meningococcemia i.e. Waterhouse-Friderichsen syndrome, APLA) and bilateral metastasis from cancer may also cause primary AI.
Secondary AI occurs as a result of depressed adrenocorticotropic hormone (ACTH) secretion leading to diminished cortisol production. Aldosterone levels remain normal because of preserved stimulation by both the renin-angiotensin axis and potassium. Secondary AI results in cortisol deficiency only. Adrenal sex hormone
production is also preserved. Intracranial disorders such as brain tumor,
pituitary disease, postpartum pituitary necrosis, or major head trauma
may affect the hypothalamic-pituitary function may lead to secondary AI. However, the most common cause of secondary adrenal insufficiency is long-term therapy with pharmacologic doses of glucocorticoids.
Clinical Features
Primary adrenal
insufficiency presents with symptoms of diminished cortisol, aldosterone, and gonadocorticoids, and elevated ACTH, which causes skin hyper pigmentation. Aldosterone deficiency symptoms
include dehydration, syncope, salt craving, and hypotension. Gonadocorticoid deficiency symptoms are decreased axillary and
pubic hair and decreased libido. Typical Primary AI presents with HypoNa, HyperK, Hypoglycemia, Hypotension.
Secondary adrenal insufficiency presents with symptoms of diminished cortisol (weight loss, lethargy, weakness, confusion, anorexia, GI distress, abdominal pain). Typically secondary AI presents as Hypoglycemia, Hypo/HyperNa, Hypokalemia, Hypotension.
In both primary and secondary AI, cortisol deficiency are seen
Initial set of bloods should include CBC, Basic metabolic panel, renal function and blood cultures. Serum Cortisol sample can also be drawn before administering steroids.
Serum cortisol
>18 mcg/dL generally rules out adrenal insufficiency.
Serum adrenocorticotropic hormone (ACTH) level measurement also helps differentiate between primary and secondary
adrenal insufficiency. A high ACTH level is seen
in primary adrenal insufficiency, but ACTH is
low in secondary adrenal insufficiency.
Treatment
- ABCs
- IV Fluid Resuscitation (May need dextrose if hypoglycaemic)
- IV Steroids once circulation is filled (Hydrocortisone 100mg IV)
- Vasopressors
- Manage Electrolytes (HyperK, Hypo/HyperNa)
- Find and treat the underlying ethology
For primary AI, abdominal CT scan may be performed to evaluate the adrenal
glands and CXR to assess for lower respiratory tract infections. For secondary adrenal insufficiency, a head CT or MRI, as well
as blood tests of pituitary hormones, may be required for further evaluation.
Take Home:
- Consider adrenal crisis in situations of unexplained hypotension, especially in patients with a history of glucocorticoid therapy.
- For a minor illness or injury, triple the daily glucocorticoid dose for 24 to 48 hours until symptoms improve.
Posted by:
Lakshay Chanana
Speciality Doctor
Northwick Park Hospital
Department of Emergency Medicine
England
No comments:
Post a Comment