Septic arthritis is a destructive disease process classically presenting as a red, hot and swollen joint. The disease has a bimodal incidence, which peaks in young children and adults over age 55 years. Unfortunately, septic arthritis is not always easy to diagnose and presentations may be subtle without classical signs, symptoms, or laboratory markers. It remains one of those cannot miss diagnosis which are always fraught with fear. Therefore, the dictum is "Red Hot Swollen joints should be tapped" to r/o Septic Joint. Fluid is then sent for Gram Stain, C/S, White Cell count and Differential count, and Crystal analysis.
Routes of Spread: Common routes of spread is hematogenous followed by direct inoculation (trauma or localised spread from a surrounding soft tissue infection)
Common Joints - Knee>Hip>Shoulder>Elbow
Risk Factors for Septic Arthritis (More abnormal joint, more likely Septic Arthritis)
- Bacteremia/systemic infection
- IVDU (may have sternoclavicular and sternomanubrial joint involvement)
- Overlying skin infection
- Diabetes Mellitus
- Arthritic Joints, Prosthetic joints
- Elderly, Immunocompromised states
- Recent joint surgery or procedure
Common Organisms
- Staph Aures 40%
- Streptocossus 30%
- GNB 20%
- Gonococcal arthritis - Most common cause of septic arthritis in the sexually active patient population. Presents as migratory polyarthritis and may involve several joints (wrist, knee and ankles), or include a rash/tenosynovitis. 4:1 female to male predominance.
Clinical Presentation (No combination of exam findings can definitively diagnose septic arthritis)
- Typical - Swollen, Red, Immobile and Tender joint
- Pain is present in about 80%. Joint tenderness has sensitivity approaching 100%
- Fever is seen only in about 50%
- Generalized tenderness with painful limitation of active and passive range of motion. Focal tenderness and pain limited to specific movements on an active range of motion testing is more typical of periarticular inflammation (skin, bursa, tendons).
Immunocompromised patients often have polyarticular involvement and present atypically. Sudden onset of pain is more suggestive of intrinsic joint pathology, such as septic arthritis.
Work up (Serum blood tests do not rule out septic arthritis)
- Synovial Fluid Analysis - Synovial fluid with a WBC count > 50,000/mm with a polymorphonuclear cell count > 90%. However, in culture-proven septic arthritis, this WBC count is reached only in 50 – 75% of cases. Therefore, lower WBC counts cannot exclude the presence of septic arthritis. A synovial fluid WBC count >100,000/mm is more specific. MRSA-associated septic arthritis (leading cause in prosthetic joints) may have lower synovial fluid WBC counts only up to 15,000 cells/μL
- Use CRP/ESR/WCC with caution - Normal levels cannot rule out septic arthritis
- Positive Gram stain can be diagnostic; however, a negative result for bacteria cannot rule out septic arthritis (sensitivity only 50-60%). Culture remains the most sensitive test (>90%).
- Presence of crystals shouldnot be used to rule out septic arthritis. Gout and Septic Arthritis can co-exist in the same joint.
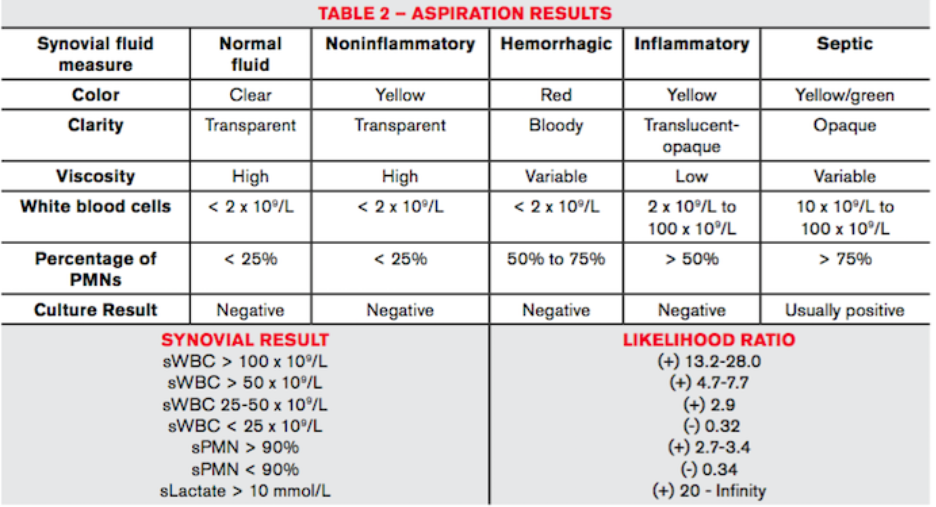
Synovial lactate has the best diagnostic accuracy in septic arthritis, based on several studies. Levels above 10 mmol/L demonstrate +LRs ranging from 20 to infinity
Imaging tests offer little assistance in the diagnosis of septic arthritis. Radiographs may demonstrate effusion or soft tissue swelling. Computed tomography (CT) has greater sensitivity for effusions and edema but is unreliable early in the disease course to evaluate for septic arthritis. Ultrasound (US) can be used to localize joint swelling and target the site for optimal aspiration.
Management
- Analgesia
- Joint aspiration
- Empiric Antibiotics (should provide gram-positive and gram-negative coverage)
- Orthopedic Referral consultation
Take Home
- More abnormal joint, more likely Septic Arthritis
- Immunocompromised patients often have polyarticular involvement and present atypically.
- Sudden onset of pain is more suggestive of intrinsic joint pathology, such as septic arthritis.
- Serum blood tests do not rule out septic arthritis
- If suspicion is still high after equivocal or dry tap, admit the patient and initiate empiric IV antibiotics while the synovial culture results
Posted by:

Lakshay Chanana
ST4 Trainee
Royal Infirmary of Edinburgh
Department of Emergency Medicine
Edinburgh
Scotland