Ulcerative colitis (UC) is a chronic inflammatory relapsing and remitting disease of the colon. The etiology is believed to be autoimmune with some genetic component. Peak incidence occurs in the
second and third decades of life with characteristic symptom of bloody diarrhoea. The rectum is almost always involved in UC.
Factors associated with an unfavourable prognosis include higher severity and extent of disease, a short interval between attacks, systemic symptoms, and onset of the disease after 60 years of age.
Clinical Presentation

Treatment
Severe ulcerative colitis - Treat with IV
steroids, fluids, correct electrolyte abnormalities,
broad-spectrum antibiotics, melamine. IV
cyclosporine (2-4 milligrams/kg per day) or infliximab (5 milligrams/kg) can be effective
in fulminant colitis nonresponsive to IV steroids.
Complications


Antidiarrheal agents, hypokalemia, narcotics, cathartics, pregnancy, enemas, and recent colonoscopy have been implicated as precipitating factors in toxic megacolon. Rx with nasogastric suction, IV steroids, broad-spectrum antibiotics active against coliforms and anaerobes, and IV fluids. Get a surgical consultation ASAP.
Disposition
Factors associated with an unfavourable prognosis include higher severity and extent of disease, a short interval between attacks, systemic symptoms, and onset of the disease after 60 years of age.
Clinical Presentation
Crampy abdominal pain, bloody diarrhea, and tenesmus are typical symptoms of UC. The disease is classified as mild, moderate, or severe depending on the clinical
manifestations.
 |
| Truelove and Witts criteria |
{kind=link}
Extra intestinal Manifestations

Diagnosis
ED diagnosis of ulcerative colitis rests on the following:
History of abdominal cramps and diarrhea, mucoid stools, stool examination negative for ova and parasites, stool cultures negative for enteric pathogens, and confirmation of diagnosis by colonoscopy.
History of abdominal cramps and diarrhea, mucoid stools, stool examination negative for ova and parasites, stool cultures negative for enteric pathogens, and confirmation of diagnosis by colonoscopy.
Treatment
Mild to Moderate attacks
Most of these patients can be treated as outpatients. A combination of oral (2.4 grams/day) and topical mesalamine is used. Topical glucocorticoid enemas or Mesalazine enemas or suppositories (500 milligrams twice a day) are quite effective in distal proctosigmoiditis and have lower systemic side-effect profiles.
If topical therapy is unsuccessful, steroids (40-60md Prednisolone/day) are effective in inducing a remission in the majority of cases. Antidiarrheal agents are generally ineffective and may precipitate toxic megacolon.
Most of these patients can be treated as outpatients. A combination of oral (2.4 grams/day) and topical mesalamine is used. Topical glucocorticoid enemas or Mesalazine enemas or suppositories (500 milligrams twice a day) are quite effective in distal proctosigmoiditis and have lower systemic side-effect profiles.
If topical therapy is unsuccessful, steroids (40-60md Prednisolone/day) are effective in inducing a remission in the majority of cases. Antidiarrheal agents are generally ineffective and may precipitate toxic megacolon.
 |
| Rx of UC based on severity of disease |
Complications
- LGI Bleed (Most Common)
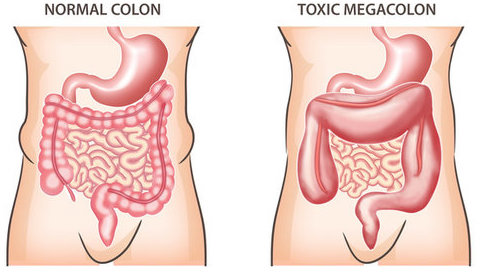
- Toxic Megacolon - The most feared complication of ulcerative colitis is the development of toxic megacolon. TM occurs as a result of extension of the inflammation beyond the submucosa, causing loss of contractility and dilated colon. Dilation of the colon is associated with a worsening of the clinical condition and development of fever and prostration. Patients with Toxic Megacolon appear toxic with distended, tender and tympanic abdomen. They typically present with fever, tachycardia and shock.

Plain radiography of the abdomen demonstrates a long, continuous segment of air-filled colon greater than 6 cm in diameter. Loss of colonic haustra represent bowel wall edema. Occasionally, features of toxic megacolon, such as leukocytosis, anaemia, dyselectrolytemia, hypoalbuminemia and peritonitis, can be masked in the patient taking corticosteroids.
- Perforation
- Bowel Obstruction (due to strictures)
- Carcinoma Colon (Advanced and prolonged disease)
- Perirectal fistulas and abscesses
Disposition
Fulminant attacks of ulcerative colitis need hospitalization
for fluid and electrolyte management and careful observation
for the development of complications. Patients with complications such
as GI Bleed, toxic megacolon, and bowel perforation
should also be admitted. In addition to toxic megacolon, the indications for surgery include colonic perforation, massive lower gastrointestinal bleeding, suspicion of colon cancer, and disease that is refractory to medical
therapy (large doses of steroids required to control the disease).
Patients with mild to moderate disease can be discharged from the
ED. It is crucial to arrange close follow-up with gastroenterologist, and any adjustment in medical therapy should be
discussed prior to discharge.
References:
- https://clinicalgate.com/toxic-megacolon/
- Oxford Handbook of Clinical Medicine
- Tintinalli's textbook of EM - 8th Edition
- http://fromnewtoicu.com/blog/2016/12/28/toxic-megacolon-1
Posted by:

Lakshay Chanana
Speciality Doctor
Northwick Park Hospital
Department of Emergency Medicine
England
This comment has been removed by a blog administrator.
ReplyDeleteHi EM Didactic Team,
ReplyDeleteMy name is Anuj Agarwal. I'm Founder of Feedspot.
I would like to personally congratulate you as your blog EM Didactic has been selected by our panelist as one of the Top 75 Emergency Medicine Blogs on the web.
http://blog.feedspot.com/emergency_medicine_blogs/
I personally give you a high-five and want to thank you for your contribution to this world. This is the most comprehensive list of Top 75 Emergency Medicine Blogs on the internet and I’m honored to have you as part of this!
Also, you have the honor of displaying the badge on your blog.
Best,
Anuj