Definition
Kounis syndrome is the concurrence of acute coronary syndromes with conditions
associated with mast cell activation, including allergic or hypersensitivity and anaphylactic or anaphylactoid insults. It is
caused by inflammatory mediators such as histamine, neutral proteases, arachidonic acid
products, platelet activating factor and a variety of cytokines released during the activation process.

Types
Type I variant: includes patients with normal coronary arteries without predisposing factors for coronary artery disease in whom the acute release of inflammatory mediators can induce coronary artery spasm without increase of cardiac enzymes and troponins or coronary artery spasm progressing to acute myocardial infarction with raised cardiac enzymes and troponins
Type II variant: includes patients with culprit but quiescent pre-existing atheromatous disease in whom the acute release of inflammatory mediators can induce either coronary artery spasm with normal cardiac enzymes and troponins or plaque erosion or rupture manifesting as acute myocardial infarction
Type III variant: includes patients with coronary thrombosis (including stent thrombosis) in whom aspirated thrombus specimens stained with hematoxylin-eosin and Giemsa demonstrate the presence of eosinophils and mast cells respectively.
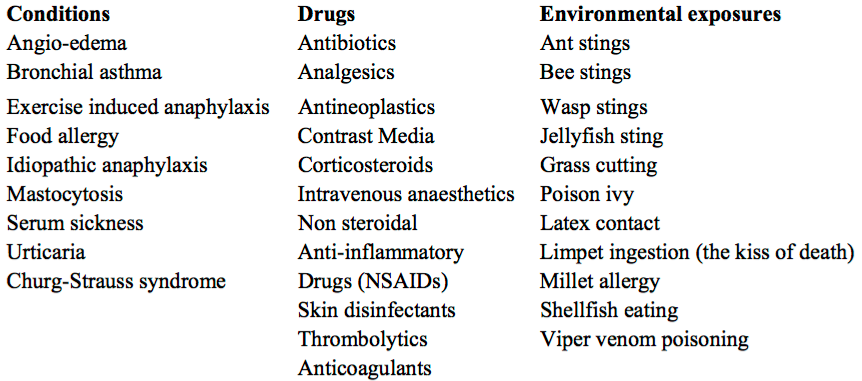
Causes of Kounis Syndrome
Treatment
•
Steroids
•
Anti-histaminics (H1 and H2 blockers)
•
Vasodilators (NTG) and routine
ACS
• Adrenaline is the drug of choice and can save lives in anaphylaxis, but in Kounis syndrome there is a chance of aggravating ischemia and worsen coronary vasospasm. Despite this risk, in severe reactions, adrenaline should be given as wide spread manifestations of Anaphylaxis are life-threatening. Sulfite free adrenaline is recommended when available. Glucagon may be considered for those who take beta blockers and do not respond to adrenaline. Fentanyl shows a slight mast cell activation as compared to morphine and
should be the drug of choice when opioid analgesia is necessary.
Posted by:

Lakshay Chanana
Speciality Doctor
Northwick Park Hospital
Department of Emergency Medicine
England
- Kounis NG, Zavras GM. Histamine-induced coronary artery spasm: the concept of allergic angina. Br. J. Clin. Pract.45,121–128 (1991).
- Kounis NG, Zavras GM. Allergic angina and allergic myocardial infarction. Circulation94,1789 (1996).
- Kounis NG, Grapsas GM, Goudevenos JA. Unstable angina, allergic angina and allergic myocardial infarction. Circulation100,e156 (1999).
No comments:
Post a Comment