The percentage of world's populations over 60 years of age will double from 11% to 22% from 2000 to 2050. As Emergency Physicians, we need to ensure that optimal care is provided to this aging population. As "kids are not just small adults", the first rule in Geriatrics is that “Elderly are not just old adults".
Geriatric population continues to increase across the world and so is the number of Geriatric ED visits. Quite often, half of the ED is occupied by elderly. It becomes a challenge to gather history from this subgroup of patients due to various reasons (sensory impairment, cognitive impairment, multiple active problems). They present late, come with subtle presentations, have an increased length of stay, frequently end up getting admitted, undergo more investigations and still face a higher mortality. Hospitals are now coming up with specially equipped "Geriatric EDs" to cater the needs of elderly.
This post mentions a few pearls highlighting the key differences between adults and elderly:
Geriatric population continues to increase across the world and so is the number of Geriatric ED visits. Quite often, half of the ED is occupied by elderly. It becomes a challenge to gather history from this subgroup of patients due to various reasons (sensory impairment, cognitive impairment, multiple active problems). They present late, come with subtle presentations, have an increased length of stay, frequently end up getting admitted, undergo more investigations and still face a higher mortality. Hospitals are now coming up with specially equipped "Geriatric EDs" to cater the needs of elderly.
This post mentions a few pearls highlighting the key differences between adults and elderly:
Abdomen
- About 1/3rd of elderly patients presenting with abdominal pain need surgery. There mortality rates are seven times higher than younger populations.
- They are less able to localize abdominal pain, less likely to produce guarding or react to rebound trigger due to poor muscle mass. They may not even complain of abdominal pain in cholecystitis, diverticulitis, or appendicitis. Don't be surprised if you end up diagnosing ACS, Diverticulitis, Intra-abdominal sepsis with a chief complaint of "weakness"!!
- Older people are less able to wall off intra-abdominal infection so they develop peritonitis earlier, even without localized pain initially. The may not give you a textbook history of disease and exact sequence of events due to underlying memory loss.
- Elderly have thin gastric mucosa and increased acid secretion so they are more likely to bleed or perforate with minimal triggers.
- Older people may not even mount a significantly increased WBC count even in the presence of a severe infection.
Dermatology
- Elderly are often less aware of pain (poor pain perception) from a skin or soft tissue infections. it is imperative to do a thorough skin exam and look for hidden abscesses, bed sores.
- Infections are easy to start, present late and slow to heal.
Genitourinary
- Close to 50% of old people have white cells and bacteria in their urine as a normal finding. Do not overcall UTI since white cells and bacteria in the urine are likely normal findings. The diagnosis of UTI should be based on new symptoms referable to the urinary tract – frequency, dysuria – OR new weakness, confusion, or falls that cannot be otherwise explained after a thorough workup.
- An elevated erythrocyte sedimentation rate (ESR) can be normal in older people. In women (age +10)/2 and in men age/2 will gives the upper limit of normal.
- A normal serum creatinine may indicate significant kidney disease. Calculate eGFR.
Cardiopulmonary
- Chest pain is rare in elderly presenting with ACS. They often present with weakness, confusion, nausea or just feeling unwell. Thus diagnosis can be delayed as symptoms sound less concerning and ECG changes are less definitive.
- Beta-adrenergic stimulation is markedly decreased with age. Tachycardia may be minimal or absent with physiologic stress. Medications such as beta blockers mask symptoms of volume loss, sepsis.
- Hypotension does not develop until much later in a hypovolemic or septic situation. 90/F with a BP of 130/80 could be in cryptic shock!
- Because of weak chest musculature and decreased airway innervation, cough is not a frequent presenting symptom of pneumonia. They may not even de-saturate until a lot of lung is not functioning;
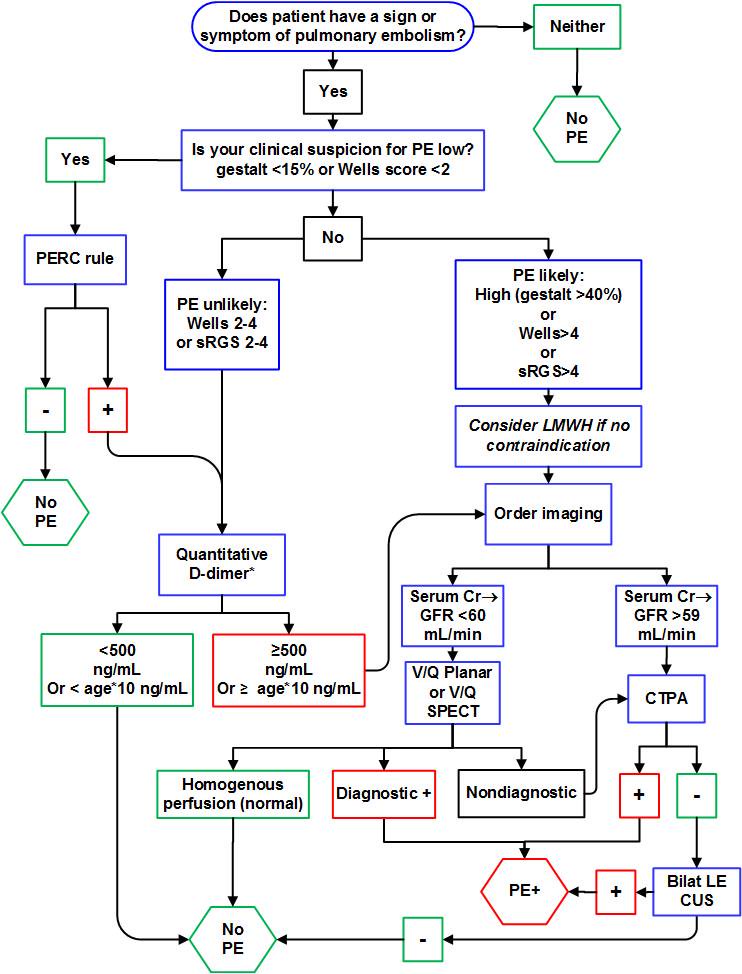
- Troponin and D-dimer can be difficult to interpret in elderly population unless “negative.”
Immunological
- The immune system produces fewer cytokines, leukotrienes and other inflammatory markers. A fever may be a very late response to infection. They can also get hypothermic with sepsis. Therefore, sepsis can present with a normal or low body temperature.
- With an infection, they often present with atypical features like "delirium" and "tachypnea" without any other obvious features of sepsis. 70% of delirium is initially “hypoactive,” which can delay its detection in the ED.
Posted by:

Lakshay Chanana
Speciality Doctor
Northwick Park Hospital
Department of Emergency Medicine
England